
Ultimate Guide to Perimenopause
TLDR: Perimenopause is the long, variable transition toward menopause with fluctuating hormones and a wide range of physical, emotional, and cognitive symptoms. This blog deep dives into many topics, including how to recognize perimenopause symptoms, how hormonal testing is limited, what treatments and healthcare approaches can help, how to find informed providers, and the positive aspects of this phase of life.
Welcome! I’m glad you’re here. If you are here, it’s probably because you either suspect you are experiencing perimenopause and aren’t sure, or because you are SURE you are and are desperately seeking resources to help. Or maybe you love someone going through this transition and are looking to learn about it (if so, go you- I’m sure your loved one appreciates it).
Our culture does an absolutely TERRIBLE job of discussing perimenopause and menopause, educating people of all genders about it, and preparing people for this important, years-long transition. I aim to be a part of the solution, not the problem, and I want to empower readers with this important information.
My intention in writing this guide is to provide a comprehensive overview of perimenopause to inform and empower women and people with ovaries so that they understand what is happening to them, learn about what might help and how to find someone to help, and explore how therapy can help in coping with this transition.
Table of Contents
What is perimenopause?
Perimenopause is the period of time when your body is transitioning towards no longer being fertile. Perimenopause usually lasts 7-14 years. It can be thought of as the mirror image of puberty, where your body is preparing to be fertile.
Menopause is reached once there has not been a period for 12 months. It is considered early menopause when the final menstrual period (FMP) is before 45 and late when it is after 54.
Perimenopause literally means “around menopause.” It begins once menstrual cycles start to become irregular and/or other perimenopause symptoms start, and it includes the first year after periods stop (much in the same way that the term perinatal means “around birth” and includes all of pregnancy and the first year after birth). However, usually when people are referring to perimenopause they are referring to the time before menopause is reached.
When do people go through perimenopause and menopause?

Most people transition through perimenopause naturally starting in their late 30’s or early-mid 40’s. You are officially in the transition to menopause when there is a difference in the length of your cycles of at least 7 days at least twice in a 10 month time span and/or when you start to experience symptoms of perimenopause (more on that below).
However, there are exceptions.
Menopause can be induced by removal of the ovaries, chemotherapy, or radiation. These folks tend to experience severe symptoms abruptly, rather than over a longer period of transition.
The term Primary Ovarian Insufficiency (POI) refers to all menopause that occurs before age 40 (about 1% of women and people with ovaries in the US). This used to be called Premature Ovarian Failure, but this name has been dropped because it is judgmental/shaming, and also because it may not necessarily be permanent or total. This diagnosis is usually discovered when people are having trouble conceiving and are pursuing fertility treatment.
If you have irregular cycles (for example with polycystic ovarian syndrome or PCOS) or you have had a hysterectomy or endometrial ablation, then changes in the menstrual cycle cannot be used to determine if you are in perimenopause. In these cases, determining what stage of the menopause transition someone is in is based on symptoms and hormonal (endocrine) tests. Testing is not recommended until 3+ months after surgery to allow hormones to stabilize. It can be difficult to determine what stage of menopause people are in who have chronic illnesses or who have undergone chemotherapy.
How do I know if I’m in perimenopause?
Perimenopause is determined by changes in your menstrual cycle and the symptoms you are reporting. If you are having changes in your cycle that are not attributable to another cause (eating disorders or illness for example), and/or you are having symptoms associated with perimenopause (more on that below), you are likely in perimenopause.
It is important to note that changes in your cycle and all symptoms of perimenopause also have many other causes, which can make it tricky to figure out what’s going on. For example, fatigue is a common perimenopause complaint, but fatigue can also be a symptom of numerous other issues. Always consult with your healthcare provider to rule out any other causes of these changes. Even if you are nearly certain it’s perimenopause, it’s good to get checked out to make sure there isn’t also something else going on.
What are the stages in the menopause transition?
There are 3 stages in the last 10-15ish years of reproductive aging, or, the transition to menopause, and 3 stages after menopause has been reached. These stages are applicable to people with ovaries regardless of demographics, size/weight, age, and lifestyle, however, they cannot be applied to people without regular menstrual cycles, those undergoing chemotherapy, and some with chronic illness.
These stages are based primarily on what is happening with the menstrual cycle. At some stages, other data such as antral follicle count (AFC- how many immature eggs are visible in the ovaries) or hormone levels. Even when hormone levels are considered, changes in the menstrual cycle are still the most important criteria.
Early Menopause Transition (Stage -2)
Cycle is off by at least 7 days (early or late) twice within a 10 month period. FSH can be elevated but is still variable, AMH and AFC are usually low. Estrogen varies wildly, even over the course of the day.
Late Menopause Transition (Stage -1)
60 or more days without a period for people 45 and older. For people aged 40-44, two episodes of 60 days without a period within a year. Menstrual cycles have more fluctuations in length and not every cycle includes ovulation. Hormone levels have extreme fluctuations between levels seen in prime reproductive years and after the final menstrual period. This stage usually lasts 1-3 years.
Early Postmenopause Transition (Stage +1a)
The first 12 months after the final menstrual period. FSH continues to rise and estrogen continues to decrease. This stage is also known as the end of perimenopause.
Early Postmenopause Transition (Stage +1b)
The second year after the final menstrual period. FSH and estrogen begin to stabilize.
Early Postmenopause Transition (Stage +1c)
Years 3-6 after the final menstrual period. High FSH and low estrogen stabilize.
Late Post Menopause (Stage +2)
Begins 5-8 years after final menstrual period and continues for the remaining lifespan. Hormones are stable and regular bodily aging is more predominant.
What are the hormones that impact perimenopause?
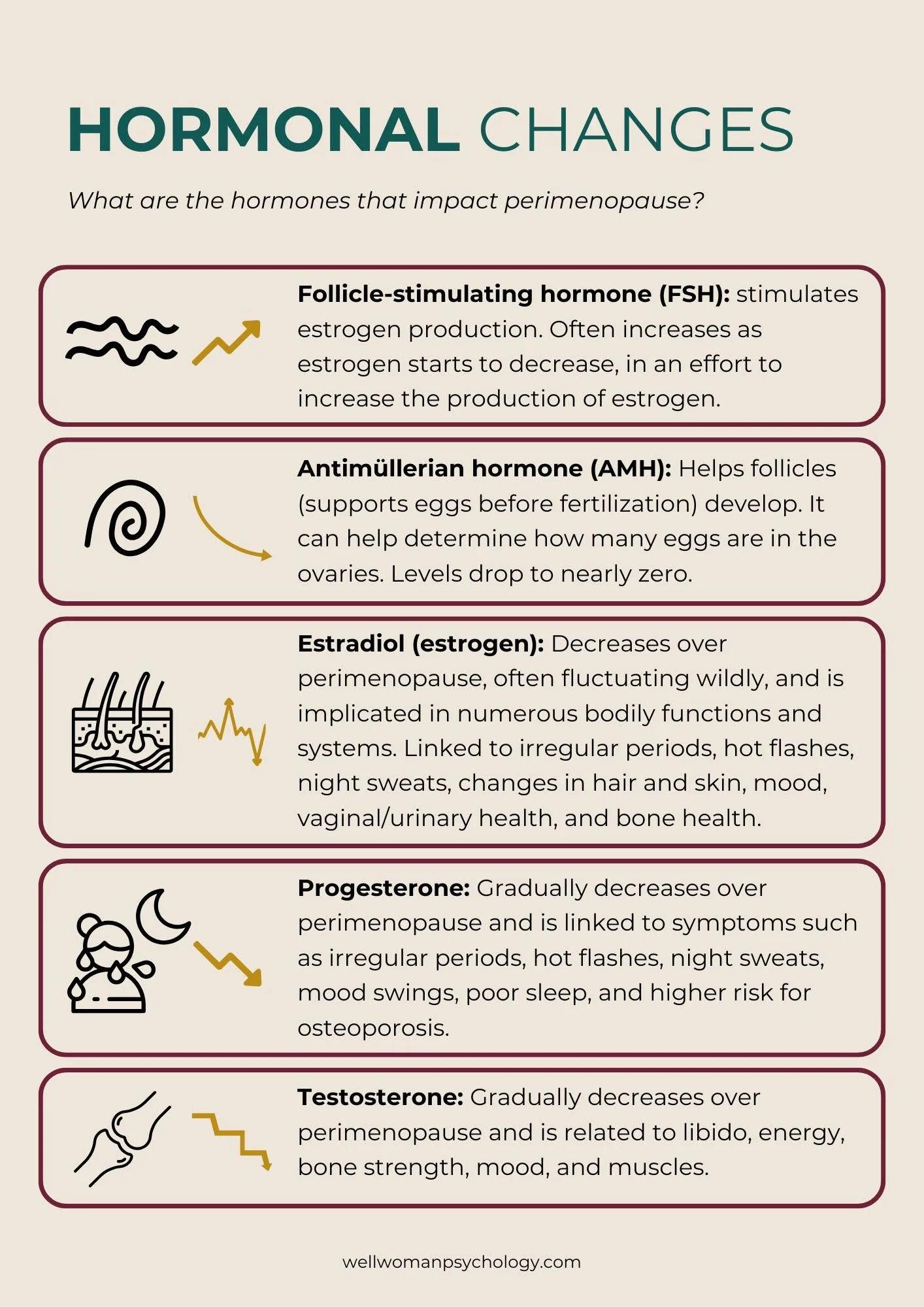
Hormonal changes that impact menopause:
Follicle-stimulating hormone (FSH): stimulates estrogen production. Often increases as estrogen starts to decrease, in an effort to increase the production of estrogen.
Antimüllerian hormone (AMH): Helps follicles (supports eggs before fertilization) develop. It can help determine how many eggs are in the ovaries. Levels drop to nearly zero.
Estradiol (estrogen): Decreases over perimenopause, often fluctuating wildly, and is implicated in numerous bodily functions/systems. Linked to irregular periods, hot flashes, night sweats, changes in hair and skin, mood, vaginal/urinary health, and bone health.
Progesterone: Gradually decreases over perimenopause and is linked to symptoms such as irregular periods, hot flashes, night sweats, mood swings, poor sleep, and a higher risk for osteoporosis.
Testosterone: Gradually decreases over perimenopause and is related to libido, energy, bone strength, mood, and muscles.
What about hormonal testing in perimenopause?
Many influencers and forums talking about perimenopause encourage women to demand regular hormonal testing, but this is not necessarily an evidence based recommendation. This is primarily because in the early stages of the menopause transition, hormone levels can vary a LOT, even over the course of the day. You might get wildly different estrogen levels testing multiple times over the course of a day for example. Also, while sometimes hormone levels may be checked, the results are not the main criteria determining what stage of menopause you are in as mentioned above.
Additionally, insurance will not cover medically unnecessary tests and, unfortunately, many unscrupulous people in the wellness industry recommend a lot of hormonal testing because it is very lucrative and the results can be used to scare vulnerable people into purchasing expensive treatments that are not evidence based. There are a lot of scam wellness interventions out there generally, and specifically in the perimenopause space as it is a trending topic these days and people are understandably desperate for insight and relief.
In short, there are times when it is helpful to test hormone levels, but it is not the key to understanding perimenopause that it is made out to be. Be wary in wellness spaces that push lots of expensive tests, especially if they are also selling “solutions.” Talk it over with a trusted healthcare provider, get a second opinion if you are unsure, and consider pressure to get expensive tests a red flag in any setting.
What are the symptoms of perimenopause?
There are MANY symptoms of perimenopause including some truly odd ones that may surprise you! Not every person has all them and they may come and go. As mentioned above, each could also have other causes, so it is always important to get evaluated to rule out other problems. I have organized these symptoms into categories the best I can.

Vasomotor symptoms (VMS):
Hot flashes (may be accompanied by sweating, chills, anxiety, or heart palpitations)
Night sweats
Heart palpitations
High blood pressure
Genitourinary Symptoms (GSM)
Genital dryness, burning, and itching
Painful urination
Increased urgency to urinate
Increased urinary tract or vaginal infections
Dry and/or painful sex
Mood and Cognition Symptoms:
Brain fog
Problems with memory
Difficulty concentrating
Lower mental processing speed
Word finding difficulty
Mood swings
Anxiety
Intense irritability or rage
Sexual and Reproductive Symptoms:
Decline in fertility
Heavy periods or bleeding between periods
Painful sex
Lack of lubrication during sexual arousal
Other:
Difficulty falling or staying asleep (often made worse by night sweats and poor sleep makes other symptoms worse)
Restless legs
Weight gain, especially in the middle
Increased cholesterol
Headache, including migraines with or without aura (visual disturbance and sometimes speech problems, tingling, or numbness)
Joint pain and stiffness (you might hear people talk about “frozen shoulder”)
Changes to skin such as thinning, spots, or wrinkles
Hair thinning (greying is not menopause related, but often overlaps with it)
Unwanted growth of hair in other areas, especially the face
Changes to body odor
Bone loss (osteoporosis)
Itchy ears
Altered sense of smell
How are women affected by perimenopause?
Women and people with ovaries may have few, many, or all of the symptoms mentioned above and these symptoms can impact each other and create or contribute to other problems. For example, nightsweats can make sleep very difficult, which in turn makes the mood and cognition problems much worse. It also can increase your risk for other health problems by itself, but also via secondary pathways, like if you are too tired to exercise, then your mood and health worsens because you are getting less movement.
Additionally, I find that it is a confusing time (which is part of the reason I’m writing this) - your body may not be behaving the way you are accustomed to and you may be confused by what is happening to you (similar to puberty!). You may have been menstruating reliabily with stable bodily processes for years, only to have it change and fluctuate, perhaps out of nowhere. This confusion can feel even more extreme for people who go straight from a postpartum period to perimenopause or get pregnant in the midst of perimenopause.
Women often experience themselves “running out of fucks to give” during this period. This sentiment is behind the viral We Do Not Care Club. However, while this can take an adjustment period to get used to, it can be a real gift! Perimenopause is an opportunity to let go of people-pleasing and the many unrealistic standards, especially in terms of beauty and mental/emotional labor, placed on women.
Mood swings and irritability can show up in relationships too. I find this usually looks one of two ways - either benign things start to annoy the heck out of you about your perfectly sweet partner (for instance, the sound of their breathing) OR the lack of emotional bandwidth makes preexisting problems harder to ignore anymore.
Changes with the body, such as weight, body composition, skin, and hair, can cause or increase body image issues and disordered eating. This is a vulnerable time for body image and disordered eating and exercise, either new onset or pre-existing struggles that are made worse by the pressures to be thin and appear young. And yet… perimenopause can be a powerful opportunity to let go of shame, guilt, and anxiety and develop a nurturing, supportive relationship with your body.
Lastly, I cannot NOT mention the nearly universal experience of being completely and justifiably frustrated in the lack of conversation around perimenopause (nobody is prepared for this!) and the difficulty in finding a healthcare provider who is both informed about perimenopause and its treatments, and who has good bedside manner and listens. If you have been dismissed or told you aren’t in perimenopause or only offered birth control - you are not alone. Most healthcare providers get little to no training in peri/menopause and many women experience being dismissed, especially women with marginalized identities. Women in larger bodies, women of color, and women with disabilities are particularly vulnerable to this and trans or nonbinary women are often left out of the conversation completely.
What treatments can help perimenopause?
Given that I am not a prescribing provider, I cannot give medical advice on medical treatments for perimenopause. However, here is a brief overview for educational purposes. If you are interested in these treatments, discuss them with your medical provider.
Hormonal birth control: can manage symptoms in some women and may be helpful for women who also want to prevent pregnancy (you are fertile up until your last menstrual period), however they are not clinically indicated for everyone and are higher levels of hormones than hormone therapy.
Hormone therapy (HT): Formerly called hormone replacement therapy (HRT), hormone therapy aims to provide some level of hormones to regulate levels and ease the symptoms caused by perimenopause/menopause. Treatment can be systemic (oral medication or a patch), or local (topical or vaginal administration). Hormone therapy contains lower doses of hormones than birth control and, like with birth control, may or may not include progestogen. Hormone therapy was discouraged for a long time because it was thought of as dangerous after the results of a major study were misinterpreted: we now know that for most women it is safe and effective in managing symptoms and often has health benefits too (i.e. lower risk of cardiovascular problems).
SSRIs (anti-depressant medication): Patients are often offended and confused when offered anti-depressants for perimenopause symptoms, but research shows that some of them are effective in reducing hot flashes, as well as of course the mood symptoms. Interestingly, some antidepressants are effective in treating extreme PMS (pre-menstrual dysphoric disorder or PMDD), which can be similar to symptoms of perimenopause.
Gabapentin: Shown in research to be effective in treating vasomotor symptoms in some women.
Soy products: Research is mixed on the effectiveness, but some women report they are beneficial.
Pelvic floor physical therapy is helpful for the genitourinary and sexual symptoms of peri/menopause.
Therapy! More on that in the next blog post.
What you do not see on the list above is weight loss. The first reason for this is because there is not a single study that shows that any weight loss strategy (including surgery and GLP1s) maintains the weight loss in the long term (5+ years). Second, pursuing weight loss has serious risks for physical and emotional health issues, including the issues it is purported to solve (for example, losing and gaining weight on diets is a significant risk factor for higher cholesterol and negative metabolic changes). Third, research has shown that weight loss is not effective for managing vasomotor symptoms.
Interestingly, people at higher weights have worse vasomotor symptoms before menopause, but much less than lower weight folks after menopause is reached.
Exercise and yoga have not been found to be helpful in managing vasomotor symptoms, but are helpful with problems such as mood, sleep, anxiety, and cholesterol. Research on the usefulness of supplements is lacking, as is testing on quality control and accurate dosing. Most of the research that does exist does not show that they are effective when compared to placebos and many have side effects. Additionally, in the US, supplements are not regulated. There are some exceptions such as omega 3 for cholesterol issues and vitamin D for mood and bone health. When in doubt, check with your doctor.
Both the American College of Obstetrics and Gynecology (ACOG) and the Menopause Society do not recommend compounded bioidentical hormones (hormones from plant sources) for most patients, due to the lack of evidence showing they are more effective or safer than hormone therapy, and the lack of regulation by the FDA, meaning they could vary significantly in terms of safety, quality, and dosing.
How do I find a provider competent in perimenopause?
Ah, the million dollar question! Unfortunately, there is no foolproof way to find someone and it really does vary by clinician. One practice might have people who are excellent in addressing peri/menopause concerns and others that are terrible. Trust your gut and if you do not feel listened to, check out my guides on how to push back on medical gaslighting or think through treatment decisions. Do not be afraid to seek a second opinion or fire a provider who does not listen to you despite attempting to clarify misunderstandings
Start by asking around - a personal referral is ideal.
The Menopause Society has a certified menopause provider credential and a directory of all their certified providers. There are also menopause focused clinics such as Midi, Alloy, and, locally, the UCLA Menopause Clinic. Experience with these clinics vary wildly - I hear rave reviews and also “meh” reviews.
The positives of perimenopause
While there are many uncomfortable parts of this massive, years-long hormonal shift, I firmly believe that there are some real upsides to this transition.
Women spend YEARS, decades even…
Disconnected from our bodies and emotions, often ignoring what they are telling us about what we need
Performing a disproportionate amount of mental and emotional labor in our relationships
Trying to shrink and fix our bodies, criticizing them and trying to make them conform
Smiling and people pleasing and stuffing our anger
Putting ourselves last

Perimenopause and its symptoms (yes, even the most hated ones) present the opportunity to reevaluate if these patterns are still serving us and if not, learn to release them and build new patterns that serve us better. People talk about women “letting themselves go” as a negative thing, but what if we reframed this? Letting go sounds like an invitation… to lower stress, better health, feeling more grounded, and increased self-compassion and space to meet our needs.
I feel that perimenopause brings us to a fork in the road - do we want to double down on trying to stuff, please, fix, and shrink? Or do we want to do the hard work to choose liberation, peace, and true self-care?
Reputable Resources and Recommended Reading:
Melanated Menopause Alliance (support and education aimed at women of color)
A Women’s Guide to Menopause, Body Image, and Emotional Wellbeing at Midlife by Signe Darpinian, out December 8th, 2025
Unapologetic Aging: How to Mend and Nourish Your Relationship With Your Body by Deb Benfield, out December 15th, 2025
Warning: MANY menopause related media (books, websites, podcasts, etc.) are full of antifat and ageist bias and push interventions that are not evidence based (weight loss, I’m looking at you) or unrealistic and harmful beauty/body standards. The two books I have listed above are weight neutral and address the body image concerns that can come up during peri/menopause.
Free Resource for Providers:
The Therapist’s Toolkit: Perimenopause & Menopause is a guide for therapists and mental health providers to help them recognize and respond to the emotional, cognitive, and physical effects of hormonal transitions.
It offers practical tools for psychoeducation, validation, and weight-inclusive, compassionate support, so clients feel understood and empowered during this stage of life.
Start Online Therapy for Perimenopause in California:
You do not have to navigate this phase of life alone - Well Woman Psychology can help. Dr. Baggett is not only an expert on perimenopause with lived experience, but she offers compassionate, liberation focused, evidence-based therapy that can help you not only cope with all the physical and emotional changes, but let go of the pressures to be perfect that may have been chasing you until now. With the right support, this can be a time of powerful transition rather than just miserable symptoms. Get support now by following these steps:
Reach out for a consultation at Well Woman Psychology.
Meet with an online perimenopause therapist in California
Start feeling supported through your perimenopause transition
About the Author:
Dr. Linda Baggett is a Licensed Psychologist and the founder of Well Woman Psychology. Serving clients virtually in California, Colorado, Illinois, New York, and Washington, Dr. Baggett has been focusing on women’s health her whole career, with experience working as a psychologist embedded in women’s primary care and OB/GYN clinics. In addition to her work on perimenopause, she helps clients to heal from trauma, relationship issues, sexuality, pregnancy loss and miscarriage, infertility, perinatal and postpartum struggles, and body image and size-based oppression. Additionally, she is trained in many evidence-based trauma treatments, including EMDR.
Disclaimer: This blog is for educational and informational purposes only, is not a substitute for individual medical or mental health advice, and does not constitute a client-therapist relationship.